Appendix D: Child death review mechanisms in Aotearoa
This section outlines the various mechanisms for reviewing child deaths from confirmed or suspected abuse, homicide, non-accidental injury or maltreatment in . Figure 6 gives an overview and more detailed information on the reviews that agencies complete is provided below this.
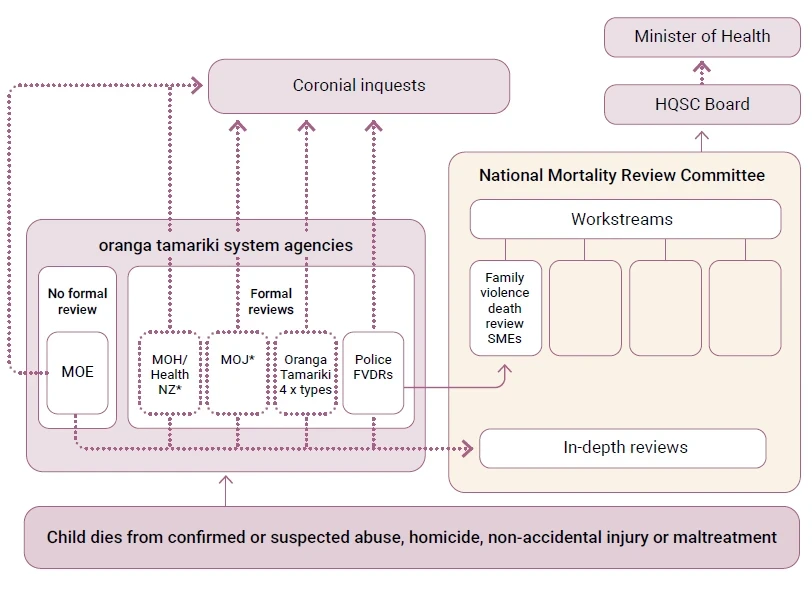
Figure 6: Process for review of child deaths from confirmed or suspected abuse, homicide, non-accidental injury or maltreatment.
* These agencies told us they do some reviews, but could not provide copies of what these reviews look like. Agencies with a dotted line do not review all of these deaths.
All child deaths where abuse, homicide, non-accidental injury or maltreatment is suspected are investigated by Police. After the investigation, Police may also undertake a review of the death. Where the suspected perpetrator is a family member, partner or caregiver, Police should undertake a Police family violence death review (PFVDR).
The purpose of a PFVDR is to help prevent future family violence deaths by highlighting improvements that could have helped prevent the death and any changes that should be made to Police practices and procedures. The reviews look at Police’s interaction with external agencies but do not examine the practices of other agencies apart from their engagement with Police and their known interaction with the parties involved, if relevant.
PFVDRs follow a set format and are completed by Police kaimahi in the district or area where the death occurred. PFVDRs are expected to be completed within 12 months of the death. As shown in Figure 6, all completed PFVDRs are provided to the Family Violence Death Review Subject Matter Experts of the National Mortality Review Committee to help inform its review function and reporting.
The death of a child who is known to Oranga Tamariki triggers the preparation of a Serious Event Notification (SEN). This is not a review of the death but a report prepared from CYRAS records. The SEN is provided to the Ombudsman under section 42(2) of the Oversight of Oranga Tamariki System Act, which requires Oranga Tamariki to provide information on all critical or serious events.60
If a child known to Oranga Tamariki or in its custody dies from any cause, Oranga Tamariki may also decide to undertake a review. The decision whether or not to undertake a review is made by the Decision-Making Forum (DMF), a group of Oranga Tamariki senior leaders.61 Sometimes, particularly if the DMF feels that Oranga Tamariki had little involvement with the child and their , a decision is made not to undertake a review.
If the Oranga Tamariki DMF decides a review is to be done, a decision will also be made about which of four types of review, with differing methodologies, will be done.
- Initial case assessment: This is led by the site involved. It is described as an initial analysis to identify practice improvement opportunities and to understand operational risks. It is typically completed within two weeks.
- Practice opinion: This is led by the Office of the Chief Social Worker. It is described as an analytical review of practice, usually in relation to a set event or timeframe. The review uses information from CYRAS but may also involve some engagement with the site and/or region within Oranga Tamariki. It does not involve interviews with anyone outside of Oranga Tamariki to elicit further information. Terms of reference will provide a timeframe for completion, which is usually four to six weeks.
- Rapid practice assessment: This is led by the Office of the Chief Social Worker. It may be undertaken on request from a critical stakeholder62 following a death of a child or or significant event where Oranga Tamariki has current and relevant involvement or very recent and significant involvement. It is described as a holistic assessment of practice related to a specific event or time period. It is intended to provide an overview of the practice and the system context in which the practice has occurred. It may include phone calls and interviews with some external stakeholders to identify any relevant information in addition to what is held by Oranga Tamariki, but it does not include engagement with or their whānau. Terms of reference will provide a timeframe for completion, which is usually eight to 10 weeks. From the reviews we received from Oranga Tamariki, this is the process it most commonly uses for reviews of child deaths.
- Practice review: This is led by the Office of the Chief Social Worker. It is described as an in-depth review of the practice that occurred with te tamaiti or rangatahi and their whānau to understand what did happen as well as what should have occurred. Practice reviews can include engagement with other stakeholders outside of Oranga Tamariki, including children’s system partners, / and family and whānau. Practice reviews make findings of fact and recommendations for change (where appropriate). They are lengthier and may take longer than other types of review by Oranga Tamariki. They are not common – the last practice review undertaken by Oranga Tamariki was the review of Malachi’s death in 2021.
The reviews appear to be used internally only. They do not appear to go to a central oversight body such as a ministerial group.
The DMF meets weekly to review and maintain oversight of workflow in relation to a death or significant event.63
A new Child Protection Investigation Unit at Oranga Tamariki will also review child deaths
The Child Protection Investigation Unit (CPIU) was established at Oranga Tamariki on 22 November 2024. The CPIU was set up in part to respond to recommendations by the Royal Commission of Inquiry into Historical Abuse in State Care and in the Care of Faith-based Institutions. When it was announced, the Minister for Children said the CPIU “reflects an unwavering commitment to learning from past failures and restoring trust in the Care System”.64
The work of the CPIU is governed by a Charter that was updated in October 2025. Its primary purpose is to improve the safety of tamariki.
While situated within Oranga Tamariki, the CPIU is operationally independent and is not part of any Oranga Tamariki site, region or service line. It is separate from existing review processes or internal investigations and reports directly to the Chief Executive of Oranga Tamariki.
The objective of the CPIU is to enhance the capability of Oranga Tamariki to care for and protect tamariki in care or known to Oranga Tamariki. It does this by providing independent, objective assurance that Oranga Tamariki is responding appropriately and in a timely manner to matters of serious concern involving tamariki.
CPIU investigations and reviews may be case specific, thematic or systemic. CPIU reports will contain findings and may make recommendations to the Chief Executive aimed at improving practice, policy and processes. The CPIU will oversee the monitoring of Oranga Tamariki responses to its recommendations to ensure timely and purposeful implementation. Following an investigation, the CPIU will share its findings and recommendations with staff to promote continuous improvement.
The work of the CPIU includes, but is not limited to:
- investigating the deaths of tamariki in care or known to Oranga Tamariki
- investigating allegations of caregivers causing harm to tamariki in care or known to Oranga Tamariki
- investigating other matters that give rise to serious concerns or where there are complex or systemic issues that pose a risk to tamariki.
The CPIU will look at whether Oranga Tamariki followed legislation, policies and practice standards correctly when it worked with a family. Its investigations will examine how Oranga Tamariki interacted with other agencies, including the operation of information-sharing protocols.
The CPIU has no jurisdiction over other agencies and will not examine the actions of other agencies or make findings or recommendations in relation to them. In our oversight role, we will watch the progress of the CPIU and its impact on strengthening the oranga tamariki system.
Health Quality & Safety Commission
The national mortality review function of the Health Quality & Safety Commission comprises:
- National Mortality Review Committee
- subject matter experts appointed to provide expert advice on the National Review Committee’s mortality review workstreams65
- a National Mortality Review Function Management Group (a division of the Health Quality & Safety Commission).
The purpose of the national mortality review function is to review and report on avoidable mortality. Its aim is to prevent future premature deaths and to promote continuous quality improvement by collecting, analysing and reviewing mortality data on specific classes of death.
The Family Violence Death Review Subject Matter Experts undertake in-depth reviews of two to four deaths each year66 on behalf of the National Mortality Review Committee. The in-depth reviews are independently facilitated and collate relevant information from across agencies, including PFVDRs. The in-depth reviews, including their recommendations, are not published. However, their findings and themes help inform substantive reports that are published by the National Mortality Review Committee.
The National Mortality Review Committee reports on its reviews to the board of the Health Quality & Safety Commission, which in turn may report to the Minister of Health. Findings from in-depth reviews are also disseminated among the agencies that took part in the review process. Schedule 5 of the Pae Ora (Healthy Futures) Act 2022 prevents the release of this information more widely.
Coroners
Coroners have a role in reviewing certain deaths in . Their role is set out in the Coroners Act 2006, which states that its purpose is to help to prevent deaths and to promote justice through:
- investigating and identifying the causes and circumstances of sudden or unexplained deaths or deaths in special circumstances
- making recommendations or comments that, if drawn to public attention, may reduce the chances of further deaths occurring in circumstances similar to those in which the deaths occurred.
Among other things, coroners decide whether to open an inquiry and/or inquest into a death. If an inquiry is held, its purpose is to make recommendations or comments that may reduce the chances of other deaths in similar circumstances. The coroner’s role is also to refer the death to other investigating authorities if it considers the public interest would be served by their investigation. The coroner does not determine civil, criminal or disciplinary liability.
We note that at the time of writing, the Coroner had an inquest underway into Malachi’s death.
The Ombudsman
The Ombudsman is also able to investigate a child death if the child dies while in the custody or care of an agency it has authority over such as Oranga Tamariki residences, youth justice facilities, supervised care, and health and disability facilities.
We note that the Ombudsman also completed an opinion into Malachi’s death.
60 The Oversight of Oranga Tamariki System Act specifies what constitutes a critical or serious event. Among other events, it includes the death of a child or young person with current or recent involvement under the Oranga Tamariki Act.
61 Members include the Deputy Chief Executive of Service Delivery, Chief Social Worker, National Commissioners, Chief Legal Officer and other support functions such as General Manager of Practice.
62 Oranga Tamariki confirmed that a critical stakeholder for this purpose includes its Chief Executive, members of the DMF, National Commissioners, Chief Social Worker, Chief Legal Officer, General Manager of Practice and Child Protection Investigation Unit.
63 Oranga Tamariki defines a significant event as the death of a child who was in care, involved with Oranga Tamariki
or recently involved with Oranga Tamariki or the death of another person by and who are in care, involved with Oranga Tamariki or recently involved with Oranga Tamariki.
64 Chhour, K. (2024, November 22). Child Protection Investigation Unit established. beehive.govt.nz/release/childprotection- investigation-unit-established
65 The National Review Committee’s mortality review workstreams include family violence death review, child and youth mortality review, perinatal and maternal mortality review, and perioperative mortality review. 66 There are only a few in-depth reviews undertaken each year because there is not resourcing available to complete an in-depth review for every death. Reviewing every death is also unlikely to furnish additional insights than a smaller number of reviews.